|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Servo Story |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Testi e immagini originali, marchi commerciali della pagina © ® ™ Maquet Getinge Group - Maquet Critical Care AB |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
"Getinge buys Siemens |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Life Support Systems" |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
"Getinge buys Siemens Life Support Systems for EUR 150 Million |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
August 18, 2003
Sweden's Getinge AB Friday said it has agreed to buy Siemens Life Support Systems, a division of Siemens Medical Solutions, for about EUR 150 million.
In addition, Getinge said it will assume net assets worth about EUR 50 million.
It said the cost of integrating Siemens LSS is expected to be at most EUR 25 million, resulting in a goodwill value of around EUR 175 million.
Assuming that the necessary approval from the relevant competition authorities is obtained according to plan, then Siemens LSS will be consolidated into Getinge's accounts from October this year.
The financing of the acquisition will be carried out using Getinge's existing credit facilities.
Getinge said Siemens LSS is expected to contribute to profits before tax of EUR 10 million-EUR 12 million in 2004 and EUR 17 million-EUR 20 million in 2005.
The long-term goal is for Siemens LSS' operating margin after goodwill to be 15%, and a business that is expected to generate sales this year of EUR 205 million.
Siemens LSS is a division of Siemens Medical Solutions, one of the largest suppliers to the healthcare industry in the world.
Siemens LSS develops, manufactures and markets ventilators and anesthesia equipment for the hospital market.
Siemens LSS is expected to generate a sales turnover of around EUR 205 million during the current financial year, which ends on 30 September.
Siemens LSS employs around 720 people worldwide, of which around 400 work at the headquarters in Solna, Sweden, where the division's center for product development, manufacturing and marketing is also located.
Siemens LSS sells medical technology equipment to around 100 countries annually, having its own sales companies on all significant markets.
Siemens LSS, along with the German company Dräger Medical, is the global market leader for ventilation machines for the hospital market, with a market share of almost 30%.
In the anesthesiology product area LSS' market share is around 6% globally and puts the company in third place after Instrumentarium of Finland and Dräger of Germany.
Over the past few years Siemens LSS has shown sound volume growth driven by successful product launches of ventilation machines.
The operating margin for current activities is around 11%."
Source: PCBnewsline |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Forty years of innovation |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
in ventilation |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The polio outbreak in the 1950s and the beginning of modern Ventilation Therapy |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In the early Fifties, the last great polio outbreak spread from North America to Europe.
Scandinavia was particularly affected by the epidemic, with more than 2.900 patients succumbing to the disease in Copenhagen alone from July to December, 1952.
At that time, mechanical ventilation was not yet available to treat the victims, who quickly succumbed to the disease as a result of respiratory paralysis.
Production of copious amounts of thick phlegm and saliva led to patients becoming cyanotic because of oxygenation failure. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
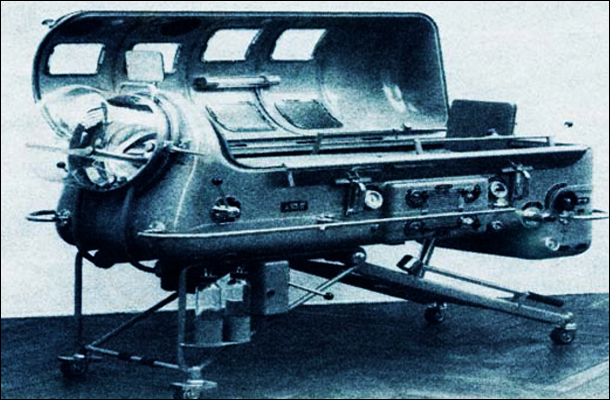
Iron lungs were considered the most advanced technology of the period, but still proved ineffective against polio |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The final stages of the disease were characterized by high temperature, high blood pressure and a high level of CO2 in the plasma.
Many patients were treated in cylindrical iron lungs, which encased the patient from neck to foot.
The iron lungs worked by applying and releasing negative pressure so that the patient's chest wall expanded during inspiration and passively contracted during expiration.
But even the iron lungs, the most advanced technology available at that time, could not save patients, and the high mortality rates continued. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
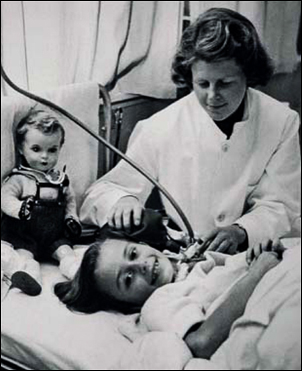
Nurses worked day and night providing manual ventilation - a tactic that saved many lives |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
At one of the major hospitals in Copenhagen, chief physician Henry Cai Alexander Lassen approached anesthesiologist Björn Ibsen to discuss possible solutions.
Based on his experience in anesthesiology, Ibsen suggested controlling the ventilation manually.
By placing a tracheal cannula, they would be able to remove secretions in the patient's airway.
A balloon was then connected to the cannula and the patient ventilated by means of manual inflation of the lungs.
As manual ventilation began to save patients in the polio wards, staff delivered bedside hand ventilation in two-hour shifts, round the clock.
Extra oxygen was given to patients from gas cylinders connected to the bags.
The doctor could control the tidal volume and the rate by squeezing the balloon, and monitor patient comfort by simply asking them how they felt. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ventilation after the epidemic The first mechanical respirators |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
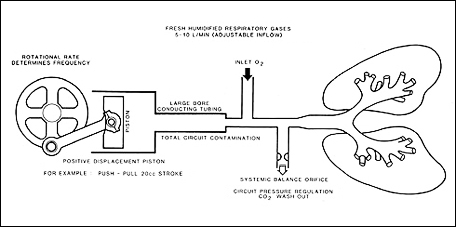
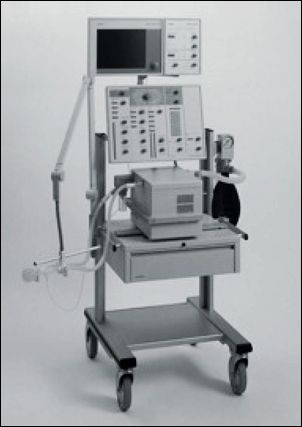
The experience with hand ventilation for polio victims soon led to the development of mechanical ventilators.
But the first generation of ventilators had several drawbacks, including being noisy and bulky.
A piston pump connected to bellows was commonly used to deliver the tidal volume, with a gearbox providing variation in the respiratory rate. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Because of their large internal compressible volume, they were not "precision" ventilators and could never be used on children.
Monitoring was only available through spot-checks, and changes in patient compliance and resistance could induce large changes in tidal volume delivery.
Sophisticated ventilation nomograms were produced, based on body weight and length, to guide the setting of the ventilator.
These nomograms usually had a "safety" margin built in, which frequently led to severe hyperinflation and hyperventilation of the patient. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Servo |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lund University Hospital in the South of Sweden had a long history of inventing ventilators, including the Barospirator (an iron lung variant) from the 1920s, Cuirass ventilators from the 1940s, and the Lundia ventilator from the 1950s.
In 1967, Clinical Physiologist Björn Jonson was busy testing what he thought was the ultimate new ventilator design.
His initial sparring partner was Professor of Otolaryngology (diseases of the ear, nose and throat), Sven Ingelstedt, who was convinced that ventilators should be flow controlled - but considered it virtually impossible to achieve.
In contrast to the design of commercially available ventilators, the new model was based on a very low compressible volume and had few moving parts.
It also featured a separate gas delivery and monitoring system with a feedback loop to accurately regulate the flow delivered to the patient.
In other words, it could be flow controlled.
Jonson knew he needed a partner with strong knowledge of modern electronics to commercialize his idea.
Sven-Gunnar Olsson, an ECG salesman at Elema-Schönander with an engineering background, joined him.
Together, they started the project to build and commercialize the first electronically controlled ventilator.
Anaesthesiologist Lars Nordström also came aboard as clinical teacher, assuring adaptation to daily clinical use as well as initial testing. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sven Ingelstedt, Björn Jonson and Lars Nordström celebrating a prototype milestone in 1970 |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Servo revolution |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The project was given a lot of freedom, and experimentation continued in an environment that fostered cross-institutional teamwork.
They also had financial support from a company that recognized the potential to add another technological landmark to their portfolio, which already included the ECG printer and the pacemaker. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
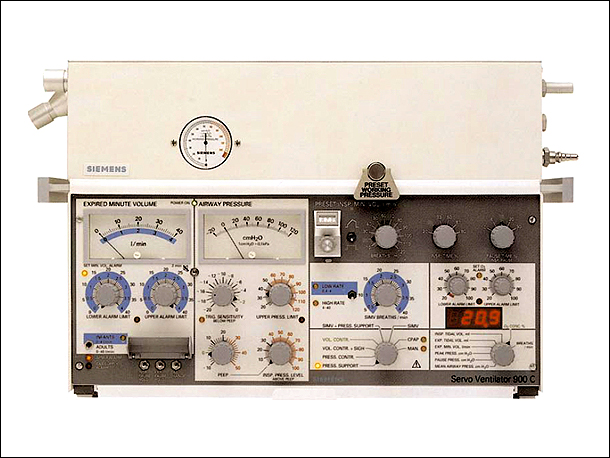
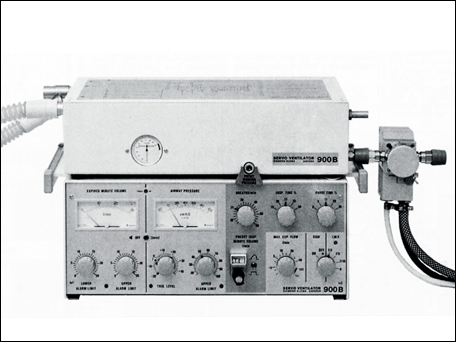
The earliest commercial version of the Servo Ventilator - "Servo 900" |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Servo 900 was introduced at the Scandinavian Society of Anesthesiologists in June, 1971 - and immediately revolutionized intensive care ventilation.
Small, silent and featuring the famous Servo Feedback System to control gas delivery, the Servo 900 meant clinicians could now reliably achieve targeted volumes and respiratory rates for individual patients.
For the very first time, the ventilator cycle could be controlled with no effect on gas delivery due to changes in resistance or compliance. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Boldly going where no other ventilator could go before |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Servo 900 really did change everything.
Maybe a little too well, especially in the beginning.
In one memorable case, the nurse at St. Eriks Hospital in Stockholm responsible for initial testing found the Servo 900 pushed into a corner on arrival each morning.
Apparently, the lack of noise caused staff to panic - they simply did not believe the machine was working!
The low noise also prompted a request from hospitals in Germany.
They insisted the Servo 900 have a small glass "window" over the pneumatic section, so they could visually confirm the ventilator was working correctly.
Nevertheless, the benefits obviously outweighed any initial concerns.
For instance, the Servo 900 was the first ventilator to display Airway Pressures, Minute Ventilation and Respiratory Rate adequately. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sven Gunnar Olsson was awarded Honorary Doctor of Medicine at the University of Lund in 1986 for his pioneering efforts in technological development and contributions to science |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The system's extensive monitoring and alarms were real breakthroughs in mechanical ventilation.
Combined with the Servo Feedback System controlling what had been set and regulating delivery, clinicians now had unprecedented treatment opportunities.
The Servo Ventilator set the standard for all modern ventilators - in fact, its unique principles are still the backbone of the Servo-i® series ventilators in use today.
Respiratory research also got a boost from the Servo 900.
By connecting the ventilator to an analog printer, it was now possible to get printouts of pressure and flow curves in real time.
This was a milestone in bedside respiratory research, and the Servo 900 became the preferred ventilator for the applied respiratory sciences. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
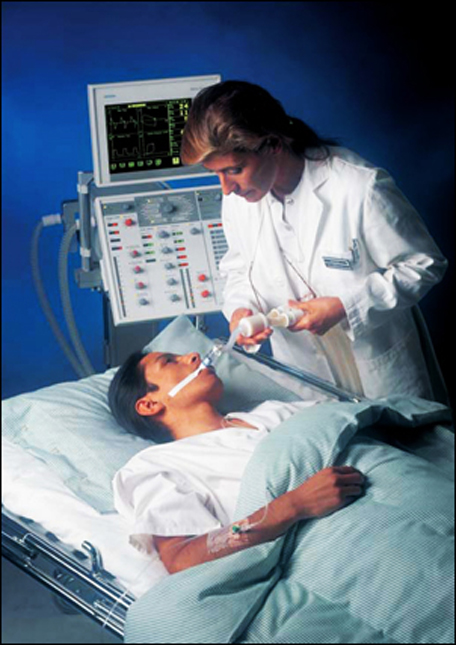
Servo offered clinicians more ventilation and monitoring capabilities, enabling its use with a wider range of patients - including children |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Naturally, the sophisticated breathing parameter settings, monitoring and alarm systems of the Servo ventilator were unfamiliar to most clinicians.
Sven-Gunnar Olsson initiated an extensive programme of training and user documentation, developed in close collaboration with researchers and hospital personnel, to bring everyone up to speed.
The user documentation and training programs of the Servo 900 and the Servo 300/PCM Patient Care Manager were awarded prizes for best practice in the industry, and their high standards are still reflected in the documentation and training development of today's Servo Ventilators. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Some of the national and international awards assigned to Servo Ventilator's User Documentation and Training Programs |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Luciano Russo, a formal teacher of Visual Communications and Non- Verbal Languages, the unconventional manager whose visionary creativity and innovative methods were warmly adopted and fully supported by Division Manager Sven-Gunnar Olsson to be successfully applied to the under many aspects "revolutionary", highly knowledge and know-how based industrial and medical project |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
He created, inspired and managed the professional team of highly skilled clinical, technical and marketing communicators which, in close collaboration with physicians, paramedical and technical staff at state-of-the-art hospitals and departments around the world, actively supported R&D and Quality Assurance in generating their traditionally functionality-focused Technical Requirements Specification - TRS rather starting the process from an innovative user and usability- centered "User Requirement Specification" - URS, resulting in the design of more user "friendly" man-machine interfaces - that is user "accessible, compatible, adaptable and supporting" at such an extent to become safe, reliable, effective, not only "easy-to-use" but "difficult-to-misuse" |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Such a "cultural" process was interdisciplinary sustained by an unprecedented in-house and on-the-field training effort all along a crucial 15-years period of time - from late 70s until the 90s - supported by condensed picture-based training material, starting from at the time poorly known "basic" Physiology of Respiration, and specific "user" documentation for sales people, maintenance technicians, ICU and OR doctors and nurses (intensive care and anesthesia) published in 8 different languages - English, German, French, Spanish, Italian and Swedish as a standard, with special editions in Russian and Japanese - greatly contributing to the worldwide success of the "Limitless Servo Ventilator System", reaching up to a 35-40 percent share of the global intensive care market |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Appointed as coaching in-house coaching consultant, Luciano Russo was soon offered to join the Ventilator Division, later Life Support Systems, at Siemens-Elema, Solna, Stockholm, at first as Information Manager (SV 900B), then Manager Marketing Communications and Manager Marketing Research (SV 900C and 900D), eventually Manager Pre-Marketing - Special Projects EV-X (SV 300 and Servo PCM - Patient Care Manager) in deep synergy with R&D and Manager User Support (SV 300) |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
After leaving Siemens in the early 90s Luciano Russo will continue to contribute to both Siemens-Elema Life Support Systems and AGA Medical Gases R&D and marketing projects through his consulting and service companies AlterEgo Informatik and AlterEgo Publishing, later AlterEgo Business Development and AlterEgo Information Design respectively, a synergetic cooperation which lasted until the mid 90s |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Servo 900B CO2 measurement comes into the mix |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In these early days and despite the changes Servo 900 ushered in, only mandatory ventilation was possible and all patients had to be heavily sedated with muscle relaxants so they could comply with the ventilator.
With experience, the world soon realized that mechanical ventilation could lead to muscle wasting, opiate dependency and barotrauma.
The next Servo introduction, 900B, specifically addressed these problems.
The new version featured Intermittent Mandatory Ventilation, allowing spontaneous breathing with machine-controlled breaths delivered at a fixed tidal volume and a low respiratory rate. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Servo 900B, the first Servo Ventilator introduced in the USA |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Servo 900B also came with a mechanical PEEP valve, which could be set by adjusting a built-in spring.
But the real breakthrough was in monitoring, when the Lung Mechanics Calculator and CO2 Analyzer 390 were introduced in 1978.
The CO2 analyzer was the first to introduce high speed infrared monitoring of respiratory gas.
In fact, the resolution of the CO2 measurement has still not been surpassed by any commercially available device.
With calculable carbon dioxide production clinicians could now measure dead space, the influence of nutritional supplementation and time dependant distribution of the tidal volume.
The analyzer saved on the need for time-consuming laboratory blood gas tests, and the end tidal CO2 value could be used to guide the setting of the ventilator. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The CO2 Analyzer 930 on top of the Servo Ventilator 900B |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CO2 monitoring made an invaluable contribution to the understanding of gas distribution in the lungs during mechanical ventilation.
It led to numerous important scientific publications and academic dissertations.
It also provided an important understanding of intravenous nutritional therapy, and frequently functioned as a metabolic monitor.
The integrated systems for lung mechanics calculation and CO2 monitoring and electronically-controlled ventilation capabilities that evolved during the 1970s paved the way for our current concepts of respiratory care. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The 1980s Re-setting the world's ventilation standards |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
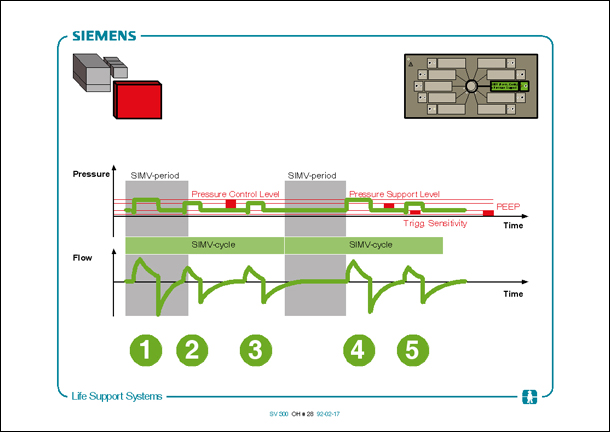
The year 1981 saw another leap forward in mechanical ventilation: the ability to deliver assistance to the spontaneously breathing patient, thanks to the Servo 900C.
A world first, the Servo 900C included a sensitive patient triggering mechanism.
Combined with the all new Pressure Support Mode, the patient could take pressure-supported breaths initiated by their own effort, which also determined the respiratory cycle.
The support was available continuously (in Pressure Support Mode), or mixed in with mandatory breaths in Synchronized Intermittent Ventilation (SIMV) Mode.
The Servo 900C also featured Pressure Controlled Ventilation and electronic PEEP adjustment. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Servo 900C the first mechanical ventilator to offer the Pressure Support mode |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The result was even more innovative treatment options for clinicians, with less risk of Ventilator Induced Lung Injury (VILI) and safer, more natural and comfortable weaning for the patient.
Another less celebrated but equally important development was humidification.
Among the first single-use HME (Heat-Moisture Exchanger) humidifier, which conserved heat and moisture on exhalation and gave it back to the patient on the subsequent inhalation, was launched for Servo 900 Ventilators in the early 1980s, eliminating the need for electrical heating. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
An 80s favourite in every department |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Magnetic Resonance Imaging (MRI) was a novel technique that emerged in the 1980s.
The environment required by the technology is a challenge for the design of the room and also for other equipment, as no magnetic items can be present.
Many patients who could benefit from an MRI examination required mechanical ventilation.
The Servo 900C had few magnetic parts, and was the first ventilator in the world to be used in this environment.
Even today, Servo remains the standard ventilator in many MRI departments around the world.
The Servo 900 series was also a highly appreciated ventilator for anesthesia.
The low pressure inlet of the ventilator allowed the pneumatics to be driven by a continuous flow, slightly above the set minute ventilation, and was a perfect adaptation in situations where ventilation needed a highly specialized type of control as in pediatrics, thoracic and neuro-surgery.
In fact, for these situations the Servo 900 became the standard and was the preferred mechanical ventilator in many European anesthesia departments.
The 900D was a late adaptation for anesthesia with improved performance and distribution of volatile anesthetics.
The Servo 900D also included a unique circle system, which allowed low flow or closed circuit anesthesia.
This advancement represented the first high performance ventilator used for the delivery of anesthesia. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
"The Limitless Servo 900 Ventilator System" |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wherever it was found, the Servo 900 series had a huge impact on modern critical care.
Its reliability and quality are legendary.
A survey done in Norway in 2000 showed that virtually every Servo 900 delivered over the years was still in use, even if some of them had been shifted out for use in veterinary institutions.
Maybe that's why so many critical care physicians still have a nostalgic relationship to the Servo 900.
And why many commercial ventilators today are still compared to it. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
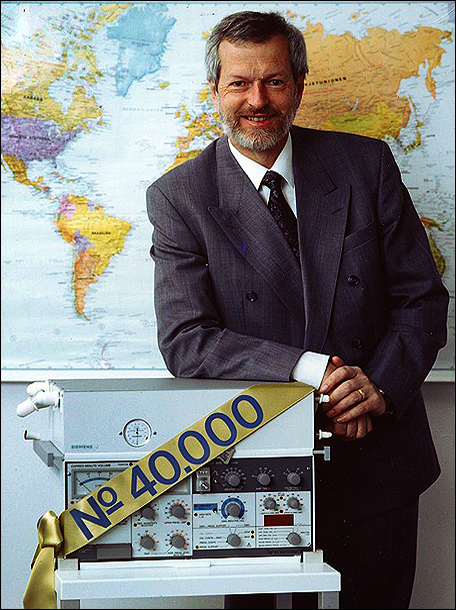
The 40thousandth Servo Ventilator 900C
ready for delivery at the Siemens-Elema factory in Solna |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A very proud Division Manager Sven-Gunnar Olsson with the 40thousandth SV 900C |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Servo 300 Leaping into the age of microprocessing |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1991 saw the introduction of an entirely new generation of Servo ventilators: the 300 series.
A giant technological advancement, the Servo 300 series took full advantage of microprocessing innovation and for the first time enabled treatment of all patient categories, from adults to neonates, using the same ventilator.
The Servo 300 series provided a completely new and unique gas delivery system with a small mixing chamber and microprocessor- controlled valves.
The fast flow response coupled with sensitive flow triggering made the Servo 300 a truly universal ventilator, allowing assisted and controlled ventilation for all patient categories.
With the advent of lung protective ventilation and the realization that Ventilator Induced Lung Injury (VILI) was a common side effect of mechanical ventilation, many clinicians started to prefer pressure-controlled ventilation in order to avoid high airway pressures and improve gas distribution in the lungs.
Others maintained that it was crucial to control tidal volumes in order to avoid fluctuations in PCO2. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
"One for all" The Servo 300 made effective mechanical ventilation available to every patient category |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
With this background, it was natural that the Servo 300 came with a new ventilation mode: Pressure Regulated Volume Control (PRVC).
This mode delivered pressure-controlled ventilation with a volume target set by the operator, and was an immediate success.
The extremely fast sensing system coupled with a prompt flow response recruited previously collapsed areas of the lungs and frequently led to continuously falling airway pressures over time.
It thus became the first true lung-protective mode of mechanical ventilation.
Its importance is reflected in the attempt by other vendors to copy it - but as they say, often imitated, never duplicated. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Working together to be better |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The ongoing development process of the 300 series was helped in a, until that time, quite unique process: close collaboration with groups of physicians.
This collaboration put a special focus on neonatal therapy and ventilation modes, the most widely viewed areas of importance in terms of therapeutic and clinical needs.
Many physicians expressed a clinical need to view bedside parameters.
The Servo Screen 390 was developed to enable monitoring of waveforms, loops and numerics at the bedside, and thereby the optimization of the ventilator settings.
Intensive care physicians were becoming very interested in nebulization, but jet nebulizers had great limitations, as they required their own bias flow to drive nebulization.
This was a complication, affecting airway pressure, volume delivery, O2 concentration and trigger sensitivity.
The Servo 300 Ventilator provided the first ultrasonic nebulizer integrated and controlled by a mechanical ventilator.
The ultrasonic nebulizer enabled the bedside delivery of drugs proportional to the flow delivery, with an average particle size of approximately 3 microns, optimal for alveolar penetration and distribution.
The non-interference with the ventilator settings was especially appreciated in neonatal practice. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accelerated research and clinical applications |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
By the mid 1990s, research on imposed work of breathing (WOB) and weaning accelerated as devices designed for bedside measurement became commercially available.
The Servo AUTOMODE® function was developed to form a bridge between controlled and spontaneous ventilation in the early weaning process. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Thanks to microprocessing technology and ongoing performance development, the Servo 300 was significantly smaller and more mobile, yet far more feature-laden, than any other ventilator that came before it |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Three controlled modes were linked to two supported modes, so the patients could wean themselves automatically with AUTOMODE.
A patient effort immediately switched the ventilator from a controlled to a supported mode, and was automatically switched back to a controlled mode upon apnea.
The benefits were clear: less sedation, less operator intervention and fewer alarms.
Weaning could be started earlier and patient activity was always rewarded without any intervention from the staff.
Lung recruitment and lung protective ventilation were areas of intense research at this time.
The migration from ventilator settings based on blood gases to using lung mechanical information is best exemplified by the implementation of PRVC. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Servo 300 NO Delivery System |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
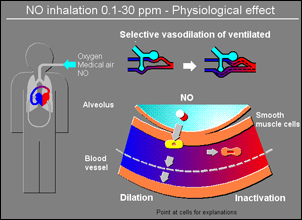
But research using the Servo 300 Ventilator, primarily in Uppsala and Rotterdam, heralded the early implementation of the Open Lung concept and the famous editorial by Professor B. Lachman: "Open up the lung and keep it open".
The discovery that Nitric Oxide (NO) was an important signalling molecule resulted in its proclamation as "the molecule of the year" in 1992, and a subsequent Nobel Prize.
The critical importance for blood flow regulation in the lung spurred intensive research in applications related to critical care.
A major practical problem at the time was the reactivity of the gas, giving rise to several well-known very toxic substances, most notably Nitrogen Dioxide (NO2).
It was found that the formation of toxic compounds was critically related to the concentration of NO and Oxygen, as well as the
design of the
delivery system. Ventilator 300 resulted in an unparalleled achievement of safe NO delivery that remains unsurpassed to this day. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Servo-i Making waves with modularity |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The previous generation's system of responding to market feedback and customer needs led to the next great advance in ventilation: The Servo-i Platform.
A modular system, Servo-i now allowed clinicians to configure the mechanical ventilator that best suited their clinical needs, while also enabling them to upgrade to new functions as they became available.
Launched in 2001, the Servo-i has consistently proven itself in clinics around the world, and has been earning praise ever since.
When awarding the 2005 Marketing Leadership Award in Global Ventilator Markets, Frost & Sullivan stated:
"Customers are demanding user-friendly and modular systems that provide clinical benefits and cost effectiveness.
Maquet's Servo-i Ventilator Platform allows for a complete spectrum of treatment strategies for all patient types, conditions and care areas to meet this need.
This combination places Maquet in an enviable position having out-edged the competition".
In 2010, Servo-i was also recognized with the Industrial Designers Society of America's Gold Design of the Decade award. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Servo-i makes it easy to configure a ventilator system adapted to the unique clinic design, including ceiling mounted version |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ongoing clinical and technological development |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
True to its initial design, new functions and improvements for Servo-i continued - and continues - to be released at a brisk pace.
The OPEN LUNG TOOL® was the first bedside method to allow for the identification of the opening and collapse point of the lung.
Using the information it provided, titration of ideal PEEP could be easily obtained, as well as the effect of any recruitment maneuver. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Non-Invasive Ventilation is one of the many capabilities that can be added or upgraded on the Servo-i Platform |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Non-Invasive Ventilation (NIV) has been incorporated in the Servo-i and received positive acclaim from clinicians, coming number one in objective evaluations of different brands.
Qualitative and protective ventilation for inter-hospital transport of patients is always a challenge.
Servo-i stands out as being a high acuity ICU ventilator conditionally approved for use in ambulances, helicopters and airplanes.
Its robustness and unique and rapid Servo control system makes it compatible with harsh environments in terms of ambient temperatures and pressures, mechanical shocks, vibrations and electromagnetic disturbances. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Servo-i supports emergency services ventilation thanks to its lightweight, robust system and easy mobility |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Servo-i has, as its predecessor Servo 900C was, been adapted to work in the MRI suite by means of a special modification kit.
And because of its excellent mobility, it can provide uninterrupted ventilation to the suite, during the examination, and back to the ICU. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A special modification kit means patients can continue to benefit from the very best ventilatory support during MRI exams |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
New lung protective tools |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Servo ventilator was the first to implement lung protective modes like Pressure Control, Pressure Support and Pressure Regulated Volume Control.
Today, the OPEN LUNG TOOL, Heliox, STRESS INDEX, and especially NAVA® (Neurally Adjusted Ventilatory Assist) have taken lung protection even further, providing critical ventilatory support with less risk of Ventilator Induced Lung Injury (VILI).
Asynchrony between the patient and the mechanical ventilator has been implicated in subtle lung injuries that lead to increased production of inflammatories.
To counter, many clinicians silence the respiratory muscles with muscle relaxants.
Others follow the accepted practice of maintaining respiratory activity even in the face of severe disease.
Either way, the ventilation strategy must emphasize lung protection.
Heliox makes it possible to prevent intubation, or buy time for patients who are difficult to ventilate.
It reduces work of breathing and oxygen demand and allows faster CO2 diffusion, giving the patient time to heal.
The Servo-i Heliox solution was designed to manage common clinical challenges of using the therapy - lowering costs and improving gas delivery. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STRESS INDEX helps identify under- and overdistension of alveoli, enabling an appropriate response to optimise compliance between the patient and Servo-i |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A complement to other lung protective features of Servo-i, STRESS INDEX helps clinicians provide gentler ventilation, irrespective of the basic ventilatory strategy chosen.
The information provided by STRESS INDEX will guide clinicians to let collapsed lung areas be allowed to rest, and avoid that open areas are submitted to cyclical stress by recruitment /de-recruitment, or overdistension if a more aggressive approach is chosen. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAVA The latest standard-setter in mechanical ventilation |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The electrical activity of the diaphragm (Edi) has always been an area of interest in mechanical ventilation.
Unfortunately, the signal quality from the diaphragm was never easy to interpret and quantitative information was impossible.
Historically, the signal could only be used to identify the neural start and stop for inspiration. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Neuro-ventilatory coupling |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
During investigation into how inspiratory muscles were recruited and what determined activity in the Edi, Dr. Christer Sinderby at the Meakins-Christie laboratory in Montreal managed what no one else could: an exceptionally high quality signal.
He knew the strength of that signal might be useful for the control of a mechanical ventilator.
But the notion of the patient's brain actually controlling a mechanical ventilator was still a little too "Star Wars": initially, little attention was paid to the technology.
But the Servo team saw its potential, and started a research collaboration.
It was easy to see why Servo-i was the perfect platform for such a project.
Its modular construction meant the extensive mathematical filtering required for signal capture could be achieved by a specific hardware module, and the ventilator assistance itself would be easily handled by the internal software design.
The result was NAVA.
And its introduction in 2007 was no thing short of a sensation.
Experts in the field of mechanical ventilation had seen NAVA and monitoring of the Edi signal as a means for physiologic study and an interesting idea.
Now it was a clinical reality and possibly a tool for treatment of patients. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Coinciding with the introduction of NAVA, scientific papers were published that showed the negative effects of patient-ventilator asynchrony, and associated to this, the problem of sedation necessary for a patient to tolerate mechanical ventilation in critical care.
NAVA has since been shown to address both these problems as, by design, there is no patient-ventilator asynchrony and the sedation requirements are substantially reduced.
The impact of NAVA and the Servo-i in neonates cannot be underestimated: the synchrony in assistance gives lower support pressures and the potential to avoid shearing forces induced by asynchronous insufflation.
Enhanced maturation of the respiratory centers, induced by the positive feedback of continued spontaneous breathing without interference, makes it possible to avoid the effects of long-term mechanical ventilation in this very sensitive patient group. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAVA literally triggers the exact assist the body requires exactly as it needs it, enabling true ventilator-patient synchrony and opening up new treatment opportunities for previously hard-to-treat patient groups |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Non-invasive, neurally-controlled mechanical ventilation, unlike traditional ventilation modes, NAVA is totally independent of leaks.
This not only makes neurally-controlled Non-Invasive Ventilation possible, it makes NIV much more effective than versions available from traditional ventilators.
Effective inspiratory assist can be given in synchronicity with the patient effort, even though constant variable leaks are present.
NIV NAVA was introduced in 2010, and has been received with overwhelming enthusiasm worldwide. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
What's next |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
New applications for NAVA and the Servo-i are being discovered every day.
The shift in treatment to patient groups traditionally treated with more invasive modes is impressive.
The notion that the patient's brain can control their own ventilatory needs, with the ventilator only providing for the lack of muscle power, is rapidly becoming the standard we can all keep building on. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Neonates with still developing respiratory systems benefit greatly from the true ventilator-patient synchrony NAVA enables |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Many of the innovations in mechanical ventilation we take for granted today are the result of an unwavering commitment to Servo development.
That is a story with no end.
As always, a focus on continuous improvement and collaboration with visionary innovators in the world of mechanical ventilation will continue to be central to Servo.
The next 40 years will certainly see many new exciting and groundbreaking chapters to the Servo story. |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In memoriam |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In memory of Sven-Gunnar Olsson 1935-2018 |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
"The difference between the impossible and the possible lies in a man's determination"
Tommy Lasorda |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
"Minnesord om Sven-Gunnar Olsson |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Företagsledaren och forskaren, medicine doktor h.c., Sven-Gunnar Olsson, Lidingö, har avlidit vid 83 års ålder.
Han efterlämnar barnen Staffan Olsson, Joakim Olsson och Johanna Hirsch, sju barnbarn, tre syskon samt stor släkt.
Sven-Gunnar Olsson föddes 1935 på en liten skogsgård nära Blomskog i södra Värmland.
Han var fjärde barnet i en syskonskara om sju.
Ungdomsårens arbete i skogen och i jordbruket lade grunden för den goda fysik som Sven-Gunnar behöll
långt upp i åren.
uppmärksammades tidigt.
12 år gammal började han på realskola i Årjäng som inackordering.
Ytterligare stipendier ledde till ingenjörsutbildning vid Chalmers i Göteborg.
Under studietiden i Göteborg träffade han Ulla, född Hultgren, sjuksköterska vid Sahlgrenska.
Sven-Gunnar och Ulla gifte sig 1957, fick tre barn, men gick skilda vägar 1977.
1960 rekryterades Sven-Gunnar till medicinteknik- företaget Siemens-Elema AB (då Elema-Schönander) i Malmö.
I branschen pågick ett teknikskifte från mekaniska till elektroniska lösningar, en bra tid för en uppfinningsrik person som Sven-Gunnar.
1967, endast 32 år gammal, utnämndes Sven-Gunnar Olsson till projektledare för Siemens-Elemas satsning på elektroniskt styrd respiratorvård.
Familjen flyttade till Sollentuna, och Sven-Gunnar började på Siemens-Elemas anläggning i Solna.
Hans utvecklingsprojekt resulterade i Servoventilatorn, som fortfarande idag är i bruk runt om i världen.
1988 promoverades Sven-Gunnar Olsson till medicine hedersdoktor vid Lunds universitet.
Han stod då på höjden av sin formella karriär.
Han var divisionschef inom Siemens-koncernen med ansvar för verksamheter i Sverige, Tyskland, USA och Japan, medförfattare till medicinska forsknings- rapporter, och upphovsman till ett flertal patent.
Doktorsgraden motiverades av pionjärarbete inom avancerad respiratorvård, teknologi som bland annat lett fram till radikalt förbättrad överlevnad för olycksoffer och för barn som fötts för tidigt.
1994 lämnade Sven-Gunnar Olsson Siemens-Elema för att ägna sig åt sitt eget företag Servotek AB i Malmö.
Företaget bedrev uppdragsforskning.
Bosättningen i Skåne underlättade för Sven-Gunnar att ägna tid åt golf.
Han var en skicklig spelare och aktiv i Ljunghusens GK och Lunds GK.
Sven-Gunnars sista tid förmörkades av demens- sjukdom.
Servotek tvingades till nedläggning.
2015 flyttade Sven-Gunnar till Lidingö för att vara nära barn och barnbarn, men hälsan försämrades snabbt.
Han fick de sista åren god omvårdnad på Siggebogården på Lidingö.
Johanna Hirsch Joakim Olsson Staffan Olsson" |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Al mio capodivisione Sven-Gunnar Olsson |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hai creduto in me, ho creduto in te.
Continua ispirazione tu, io stimolante "scheggia impazzita".
Ciascuno a suo modo, abbiamo fatto "storia" alla Siemens, circondati da sincero e mai celato odiamore-ammirazione - come è giusto che sia.
Ciascuno a modo suo, visionari troppo difficili per essere soltanto mediocramente benvoluti, meglio piuttosto tollerati.
L'esagerato mazzo di rose rosse (!) fattomi trovare sulla scrivania una mattina, inusuale quanto gradito segno di apprezzamento per il nostro contributo ai successi aziendali...
lo restituisco con immutata stima e gratitudine - te lo meriti.
Grazie di tutto!
Luciano Russo |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|